Within Four Walls
The Psychological Ideology of Post-Acute Infection Syndromes Casts a Long Shadow

“The history of human civilisation is littered with examples of natural phenomena, including human disease, initially explained by dogma. The dogma is initially created to fill a void in comprehension, but it is eventually replaced by rational scientific understanding. The creators of such dogma are often authoritarian, hierarchical figures who then ferociously defend their own creation.”
~ William Weir and Nigel Speight | 2021
Around the mid 1850s, Ignác Fülöp Semmelweis and Florence Nightingale led the way in advocating handwashing to prevent infections, yet it took over a century for their practices to gain widespread acceptance. Meanwhile, John Snow challenged prevailing beliefs about cholera transmission, contending that it was through contaminated water rather than foul odours. However, it wasn’t until nearly three decades later until this revelation was definitively confirmed.
There were other times when the medical field made significant mistakes, especially in believing mental issues caused physical illnesses. For example, Parkinson’s tremors were once believed to come from suppressed desires, and multiple sclerosis was known as hysterical paralysis until they invented the CAT scan machine. More recently, it was believed that stress caused stomach ulcers, until it was proven that a bacteria called Helicobacter pylori was the real cause.
Even today, some in the medical field stick to old ideas resisting scientific advances. A prime example of this is blaming psychological factors for chronic disease processes triggered by post-acute infections.
A mystery illness with a plethora of titles
Epidemic outbreaks and sporadic cases of a mysterious, debilitating illness with neurological-related symptoms have occurred since at least the 1930s, however it was likely occurring much earlier. Some physicians and medical historians believe that Florence Nightingale herself may have fallen victim to these same symptoms after being struck down with “Crimean fever” in 1855. She became mostly bed-bound and never recovered.
The first recorded outbreak of this poliomyelitis-like disease was in 1934 in Los Angeles and was thought to be Atypical Polio. Iceland had similar outbreaks throughout the 1940s and 1950s, commonly known as Icelandic Disease.
It wasn’t until 1956, Dr. A. Melvin Ramsay formally coined Sir Donald Acheson’s selected name for the disease myalgic encephalomyelitis (ME) in a paper describing the 1955 epidemic among staff at Royal Free Hospital in London.
The same year, researchers published their observations in The Lancet, noting a “pattern of abnormalities in spinal cord fluid and brain ganglia in patients.” Subsequently, ME has maintained its official classification as a neurological disease by the World Health Organization (WHO) since 1969 (ICD 10 G93.3).
15 years after the Royal Free Hospital outbreak, two male psychiatrists carelessly labeled this highly debilitating disease as “mass-hysteria” without even meeting any patients. McEvedy and Beard proposed their hysteria hypothesis solely because most affected individuals were women.
“It wasn’t science. It was misogyny.”
~ George Monbiot, British author and columnist at The Guardian.
Evaporation of a discrete illness “desirable outcome”
Following the 1984 ME outbreak in Incline Village, Nevada, the Centers for Disease Control (CDC) proposed the term chronic fatigue syndrome (CFS) in 1987. The subsequent year, the formal title was established with the introduction of the Holmes definition (also known as the 1988 CDC criteria). The term chronic fatigue syndrome has since been widely used and trivialised this life-altering condition.
“I think that was a big mistake because the name, in my opinion, and the opinion of a lot of people, it both trivialises and stigmatises the illness. It makes it seem unimportant, maybe not even real.”
~ Dr Anthony Komaroff, part of the CDC team who coined the name chronic fatigue syndrome.
In 1991, the Oxford Criteria broadened the diagnostic criteria for chronic Fatigue Syndrome (CFS), focusing on psychological and lifestyle factors, neglecting physical abnormalities and the defining feature of ME, post-exertional malaise (PEM).
In 1994, PEM was included in the Fukuda Criteria (1994 CDC), but it was not mandatory, risking misdiagnosis. That same year, Dr. Stephen Straus, who believed women could avoid the woes of CFS if only they were “less ambitious” attempted to bury ME altogether.
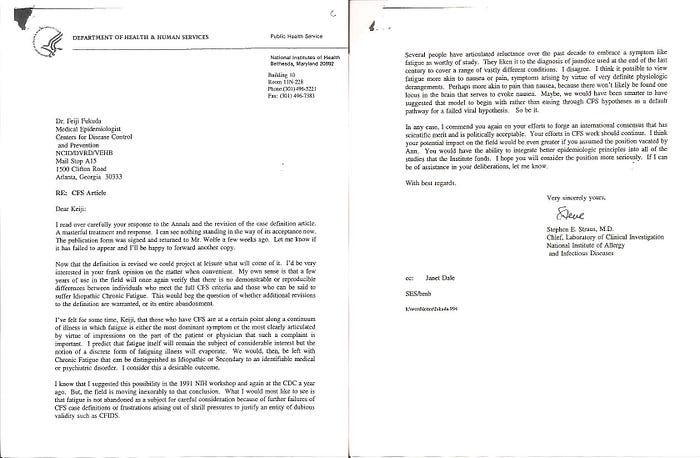
A letter obtained by ME advocate Craig Maupin via a FOIA request (Freedom of Information Act request), was sent from NIH’s Dr. Stephen Straus to CDC’s Dr. Keiji Fukuda in 1994. Below is an excerpt expressing a desire to “evaporate” ME as a distinct illness, merging it with unexplained chronic fatigue.
“My own sense is that a few years of use [with the Fukuda definition] in the field will once again verify that there is no demonstrable or reproducible differences between individuals who meet the full CFS criteria and those who can be said to suffer Idiopathic Chronic Fatigue. This would beg the question of whether additional revisions to the definition are warranted, or its entire abandonment. I predict that fatigue itself will remain the subject of considerable interest but the notion of a discrete form of fatiguing illness will evaporate. We would, then, be left with Chronic Fatigue that can be distinguished as Idiopathic or Secondary to an identifiable medical or psychiatric disorder. I consider this a desirable outcome”.
– Dr. Stephen Straus — NIH | 1994
The combination of a vague diagnostic criteria and the name change to chronic fatigue syndrome, allowed psychiatry to dominate the field with questionable therapies.
“When the full history of ME is written one day we will all be ashamed of ourselves”
~ Professor Dr. Ola Didrik Saugstad, Professor of Paediatrics and WHO Advisor
Hijacking WHO Classified Neurological Disease
UK professors Simon Wessely, Peter White and Michael Sharpe, with links to the insurance industry and UK’s Department for Work and Pensions (DWP), also played a role in sweeping ME under the rug. Sharpe expressed concern about the costs of laboratory investigations and immunological treatment.
“The use of extensive laboratory investigation may be psychologically harmful to the patient by reinforcing their beliefs about serious physical disease…. Even if shown to be beneficial (immunological) treatment is unlikely to be feasible on a wide scale because of cost.”
~ Michael Sharpe | 1991
Classified DWP documents from 1993, which were unprecedentedly stamped closed until 2072, reveal that psychiatrists Simon Wessely and Peter White opposed repositioning ME as neurological in the Disability Handbook. Instead, these psychiatrists advocated for merging ME and CFS, lending their support to CFS treatments such as graded exercise therapy (GET) and cognitive behavioural therapy (CBT), which they themselves had played a role in developing.
In documented correspondence, Wessely’s endorsement of McEvedy and Beard’s misogynistic “mass hysteria” theory appeared to be warmly embraced by the DWP, and Wessely dismissed the studies Dr. Charles Shepherd cited highlighting brain abnormalities and persistent viral presence as purely ME lobbying. However, a closer look at the classified documents clearly revealed who was lobbying whom.
“CFS/ME is defined as a psychosocial illness by the Department for Work and Pensions (DWP) and medical insurance companies. Therefore claimants are not entitled to the higher level of benefit payments. We recognise that if CFS/ME remains … defined as psychosocial then it would be in the financial interest of both the DWP and the medical insurance companies.”
~ A 2006 report by the UK Parliamentary Group on Scientific Research into Myalgic Encephalomyelitis
It’s undeniable that separating ME from CFS, and correctly classifying it as a neurological disease, would pose challenges and costs, affecting the government benefits scheme, the insurance industry and psychiatrists’ careers. All parties involved would benefit from ME being classified as a psychosocial illness, and their continued contradiction of the World Health Organisation’s (WHO) recognition since 1969 contributed to the erasure of this serious neurological disease.
“I take no pleasure in, and set no store by, the suggestion that Professor Wessely effectively hijacked the WHO logo to give credence to his own view of ME as a mental illness. Nevertheless, I am uncomfortable that the professor does not appear to be doing his utmost to clear the air on this issue.”
Wessely and colleagues fraudulently manipulated the WHO guide, changing ME’s classification from a physical neurological disorder to a mental health illness. In September 2001, the WHO corrected this misclassification, but the damage had been done. Disability support and services for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) patients in the UK were denied, with some patients placed in psychiatric wards. Consequently, eighty percent of UK doctors incorrectly believe that ME or CFS is a mental health condition.
“It’s only human for doctors to view the public as foolish, uncomprehending, hysterical or malingering”
~ Professor Sir Simon Wessely | 2003
At a lecture in British Columbia, Wessely mocked ME and CFS patients, denying the existence of their physical illness. This led to laughter from hundreds of medical professionals, at the expense of vulnerable patients. Witnessing this, Dr. Byron Hyde was dismayed by Wessely’s success in convincing physicians that these patients could return to work despite their severe disabling symptoms. The aftermath saw insurance companies using the lecture to deny benefits, causing distress among patients.
Sir Wessely has a history of blaming psychological explanations for physical illnesses. He attributed Gulf War Illness (GWI) to “anxiety about chemical weapons,” despite evidence pointing to exposure to toxic substances like sarin nerve gas. Similarly, he attributed health issues from water contamination in Camelford, England in 1988 to psychological factors. The UK government formally apologised in 2013 for the contamination, acknowledging aluminium sulphate’s role. In 2023, Wessely suggested the Iranian schoolgirl poisonings were a case of “mass sociogenic illness,” and attributed post-9/11 health problems to fear of the physical environment. However, individuals were exposed to harmful particles and debris, causing disorders like airway problems, digestive issues, and cancers.
Given the compelling scientific evidence going back decades disproving Sir Wessely’s claim that ME was a somatoform disorder, his receipt of an award for “standing up for science” in the ME/CFS field has rightfully drawn criticism. The Science Media Centre (SMC) nominated Wessely for the award, which appears a little conflicted considering Wessely was a founder member and on the board of trustees of the SMC.
The SMC propaganda machine has often discredited patients by parroting Wessely and Sharp’s poisonous words to media outlets, painting ME patients as “militants”, “malingerers” and “the undeserving sick.”
“Greatest medical scandal of the 21st century”
In 2011, the most expensive and influential ME/CFS research to date, costing £5 million, based on flawed science and deception, was published. It is crucial to observe that The PACE Trial was part-funded by the UK’s Department for Work and Pensions (DWP).
“This will emerge as one of the greatest medical scandals of the 21st century… A trial which claimed exercise helped the estimated 250,000 sufferers of the devastating illness, M.E., (myalgic encephalomyelitis) to recover was deliberately flawed to remove people from long-term benefits and reduce the welfare bill.”
~ Carol Monaghan, MP, during a parliamentary debate in Westminster.
Following Australian patient Alem Matthees’ completion of graded exercise therapy and cognitive behavioural therapy as requested by Centrelink for disability support access, he experienced a significant decline in his health. This prompted him to question the efficacy of these therapeutic interventions, which had been endorsed as curative “evidence-based” treatments by the authors of the PACE Trial.
In 2014, Alem’s freedom of information (FOI) request for PACE Trial data was denied, prompting a legal battle costing £250k, until courts ruled in his favour in August 2016. Over 100 experts criticised PACE Trial flaws, including altered recovery thresholds and misrepresented recovery rates.
A thorough analysis was made of the PACE Trial along with similar trials, and all reports found that graded exercise therapy (GET) and cognitive behavioural therapy (CBT) were ineffective long term, and GET showed potential harm.
“…many of the activists trying to have scientific papers they don’t like retracted are not patients. Patients would surely be too ill to produce so many complaints and FOI requests to journals, funders and universities.”
~ Professor Michael Sharpe, co-author of the PACE Trial tweeted | 2018

For 7 years, Alem has remained confined to his dark bedroom, too ill to read, watch TV, or socialise online. He’s too weak to change his clothes and can no longer talk or write.
Sharpe deleted his tweet after receiving a letter signed by over 100 members of the Australian ME/CFS Community explaining the profound illness these patients, Tom Kindlon and the late Robert Courtney, had endured during their immense contributions. Especially Alem, who greatly struggled with his condition throughout the FOI requests, risking all of what was left of his health with his consequent deterioration afterwards.
“The many wrongs committed by psychiatry and medicine to the ME/CFS community can only be righted when the PACE Trial is ultimately seen for what it is: a disgraceful confidence trick to reduce patient compensation payments and benefits.”
~ David Marks, Editor, Journal of Health Psychology

New outbreak with a new name “long COVID”
Early 2020, patients and researchers predicted at the beginning of the pandemic that a tsunami of post-COVID-19 sequelae would follow. Studies suggest nearly 50% of long COVID patients are now meeting the criteria for ME/CFS.
Frustratingly for ME/CFS researchers and advocates, many medical journals and media outlets referred to the lingering coronavirus symptoms as an enigma. With headings like “Long Haulers” Stump Experts, mysterious symptoms of “long COVID”, and Puzzling after-effects plaguing “long-haulers”. Canary journalist, Steve Topple, was the first journalist to connect the dots back in March, 2020.
In July 2020, Dr. Anthony Fauci said post-COVID Syndrome “Is Highly Suggestive of” Myalgic Encephalomyelitis. His following statement gave hope to millions who had been suffering for decades with the debilitating disease.
“We’ve been chasing myalgic encephalomyelitis and chronic fatigue syndrome without ever knowing what the etiologic agent was. Now we have an absolutely well-identified etiologic agent that should be very helpful now in getting us to be able to understand it. I hope we do; it’s been mysterious to us for years. Maybe this will give us a chance at a breakthrough.”
US Congress provided The National Institute of Health (NIH) with a promising $1.15 billion into long COVID research, most of which went to observational studies rather than clinical trials for treatments. If it weren’t for the recent injection of $500 million from the Biden administration, RECOVER would have been on the brink of having to close its 80 clinical sites and research endeavours.
Given the NIH’s track record, funding might lead to more dead ends than breakthroughs. RECOVER prioritises broad studies over depth, lags in staying current with long COVID research, and lacks effective fund utilisation and flexibility. Additionally, it overlooks valuable lessons from diseases like ME/CFS and doesn’t appear to be prioritising biomarker-based research. Major pharmaceutical companies are likely hesitant to engage due to the lack of robust clinical criteria. The absence of reliable biomarkers remains the primary obstacle in addressing long COVID and runs the risk of repeating the same mistakes made with ME/CFS.
The utilisation of Graded Exercise Therapy (GET) as a primary treatment method in Long COVID rehabilitation centres across Australia and other countries is a cause for concern. GET has historically been employed as a treatment for individuals with ME/CFS under the misguided belief that symptoms primarily stem from deconditioning. Despite its disuse in the US and UK due to lack of efficacy, GET persists in Australia and receives support from the government’s appointed advisor who has a commercial interest in the controversial therapy. Now, this same flawed approach is being applied to the treatment of Long COVID patients in Australia, posing significant risks to the well-being of around 50% of those who experience post-exertional malaise (PEM).
The Medicine War Continues
Decades on, those from a faction of the medical establishment who played pivotal roles in the development of graded exercise therapy/cognitive behavioural therapy (GET/CBT) and the discredited PACE Trial, maintain their resistance to emerging scientific findings.
They “ferociously defend their own creation” even after a comprehensive reanalysis discredited GET and CBT research from the PACE Trial and Cochrane Review. The therapies they continue to promote as “evidence-based,” not only fail to show long-term effectiveness, but studies now indicate they can actually trigger post-exertional malaise (PEM), causing long-term or permanent harm to those experiencing it.
Both the US Centers of Disease Control (CDC) and the UK National Institute for Health and Care Excellence (NICE) have adapted their guidelines to reflect evolving understanding, notably by removing GET in 2017 and 2021, respectively.
While these changes mark important milestones in the paradigm shift towards a greater emphasis on biomedical science in the understanding and treatment of ME/CFS, millions of patients still suffer under the shadow of dogma. This extends to the close to 50% of long COVID patients who have developed ME/CFS.
An opinion piece from proponents of GET/CBT criticising the NICE guidelines has swayed some journalists and ill-informed medical bodies. Yet, it’s hard to overlook the glaring conflict of interest evident in the authors’ extensive list of competing interests.
In response, NICE has refuted the critics’ assertions. Additionally, Professor Brian Hughes, from the University of Galway, meticulously dissects eight myths — or perceived anomalies — and addresses the prevalence of misinformation surrounding the new NICE guidelines in his presentation.
Despite the dissemination of misinformation, some doctors and hospitals remain unwilling to adhere to the updated NICE guidelines. Unfortunately, UK hospitals are not legally obligated to implement these guidelines, leading to continued harm to patients. In the midst of this, Millie and Carla, two young women, endure mistreatment from uninformed hospitals. Tragically, two other young women, Merryn Crofts and Maeve Boothby-ONeill, have lost their lives due to alleged medical negligence stemming from this refusal to accept ME/CFS as a serious disease. Their stories echo the dire situation faced by Millie and Carla today.

Sophia, Merryn, Alison, Maeve, Emily and Lynn might be alive today if resources and education hadn’t shifted from biomedical science to controversial psychosocial therapies. Autopsy findings from some of these women revealed inflammation of the dorsal root ganglia. This is consistent with other autopsies of ME patients, some of which have shown evidence of viruses in tissues of the brain and other organs. The 1956 study, I mentioned earlier, was on the right path before ME was evaporated by governments to hedge costs and hijacked by psychiatrists to win grants. These young women were doubted, mistreated, and neglected by the very healthcare system meant to help them.
Unveiling the shadows
“The last 60 to 70 years of attempts to treat this disease with psychological management and exercise have failed miserably. There is “not a single” peer-reviewed study that shows that cognitive behavioural therapy (CBT ) or so-called graded exercise therapy (GET) play any role in healing people with ME/CFS or long COVID which has not been completely discredited by serious scientists. Behavioural therapy and exercise therapy are nevertheless tools that are used, because they are cheap, and therefore attractive to governments.”
~ David Putrino, Ph.D. in neuroscience, professor of rehabilitation and human performance. Named Global Australian of the Year for his contributions to healthcare in 2019.
The journey through the annals of medical history reveals a narrative of medical progress marked by the struggle against entrenched ideologies. Yet, even in modern times, the presence of psychosomatic explanations continues to cast a long shadow over the field of medicine.
The saga of myalgic encephalomyelitis (ME) and chronic fatigue syndrome (CFS) epitomises this struggle. From the earliest outbreaks of the illness to the contemporary challenges posed by long COVID, the journey has been fraught with misclassification, misinformation, and mistreatment. The renaming of ME to CFS and the promotion of therapies like graded exercise therapy (GET) and cognitive behavioural therapy (CBT) based on flawed research exemplify how entrenched dogma can hinder progress and perpetuate harm.
Despite advancements such as the revision of guidelines by institutions like the CDC and NICE, resistance to change persists. Some within the medical community continue to adhere to outdated beliefs, resulting in ongoing suffering for patients such as Millie and Carla. Tragically, lives have been lost due to alleged medical negligence stemming from this refusal to accept the seriousness of ME/CFS.
As we navigate the complexities of post-acute infection syndromes like long COVID, it is imperative that we heed the lessons of history. We must remain vigilant against the allure of dogma and prioritise evidence-based approaches that place the well-being of patients above all else. Only then can we hope to overcome the shadows of the past and usher in a new era of understanding and compassion in medicine. ⏹
